

Dystonia is a movement disorder characterized by sustained or intermittent muscle contractions causing abnormal, often repetitive movements, postures, or both. Dystonic movements are typically patterned, twisting, and may be tremulous. Dystonia is often initiated or worsened by voluntary action and associated with overflow muscle activation1.
A patterned movement is one which is characterized by the recurrent quality of one movement being similar to the movements which precede and follow it.
The use of the term intermittent is included in the definition because there is a common misconception that dystonic movements are always sustained, slow, or twisting2. Since the diagnosis of dystonia is based on clinical observation and there are no supportive laboratory measures3, clinical recognition is more difficulty when dystonic movements occur in isolation, and these movements may include two broad categories, which are not isolated, but overlap:
- A tonic component, that is, dystonic postures, which appear relatively fixed, for example cervical torticollis.
- A phasic component, that is, dystonic movements are present, which are recognized by the examiner as being rapid and jerky:
- Dystonic Jerks: dystonic movements which affect the hands, head, or other body parts may be very brief, resembling myoclonic jerks. Examples include the periocular spasms of blepharospasm, and voice breaks of laryngeal dystonia4.
- Dystonic tremor: dystonia associated with tremor. Dystonia may even manifest as an isolated tremor without other clues suggesting dystonia.
The current definition emphasises that dystonic movements tend to be patterned, and that dystonia characteristically worsens with voluntary action. Some of the most important features of dystonia, that distinguish it from other hyperkinetic disorders, are the relationship to movement and posture, and the stereotyped or patterned character of the movements1. Some forms of dystonia, such as blepharospasm and laryngeal dystonia, are not associated with postures, but are limited to focal involuntary contractions.
Dystonia may be inherited or acquired:
- Inherited dystonia is divided into two groups: isolated dystonia (with or without dystonic tremor), and combined dystonias (dystonia plus parkinsonism or myoclonus).
- Acquired dystonia can occur from damage to essentially any component of the motor system, though is classically associated with putaminal damage. Many pathologic processes that damage motor circuits can cause dystonia, including neurodegenerative disease, stroke, and trauma5.
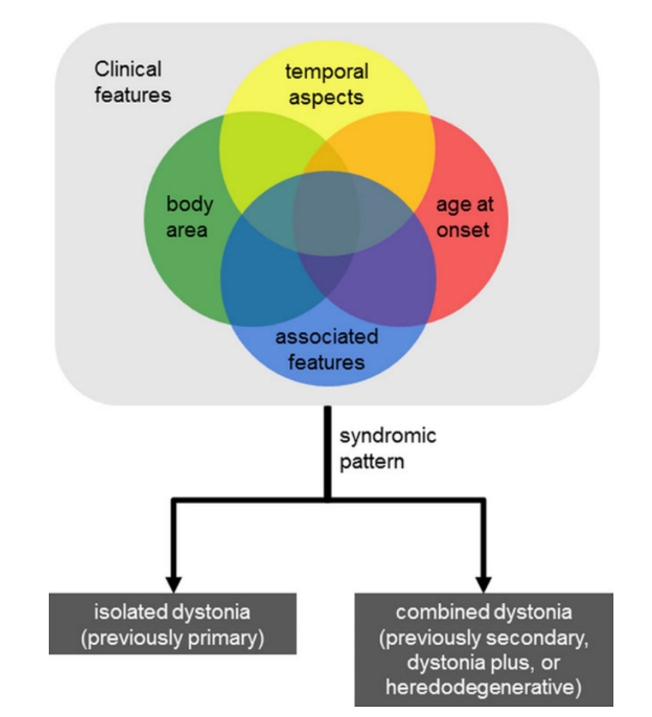
Current classifications of dystonia take the approach of reviewing the clinical features, and then using these, subsequently to determine the syndromic pattern (see Figure) 2.
Women are affected by dystonia about twice as often as men. Although the genetic causes of dystonia, especially for adult-onset focal forms, are still largely elusive, a positive family history is found in about 20% of dystonia sufferers3.
From: Jinnah HA, Albanese A. The New Classification System for the Dystonias: Why Was It Needed and How Was It Developed? Mov Disord Clin Pract. 2014;1(4):280-284. doi:10.1002/mdc3.12100