

Laterocollis Laterocaput Lateral Shift

Distinguishing between laterocollis and laterocaput is clinically possible, without the need for additional tests, such as CT or MRI of the cervical spine.
Laterocollis
If muscles are involved whose sites of origin or insertion lie between C2 and C7, this will result in the neck being flexed, corresponding to laterocollis. In this case, the head and neck are in the same plane.
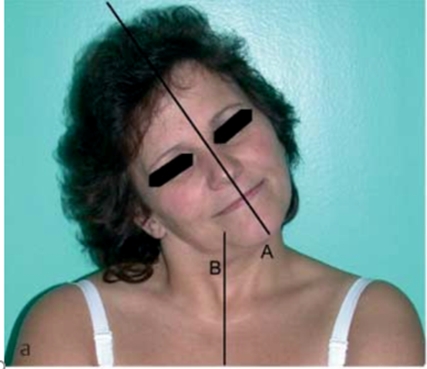
Laterocaput
Dystonia of the muscles which have their sites of origin or insertion in the skull or the first cervical vertebra, results in an abnormal posture which is limited to the head only, and where the cervical spine is normal.
Combinations of laterocaput and laterocollis are commonly found1.
Distinguishing laterocaput and and laterocollis
It is usually possible to differentiate clinically between laterocollis and laterocaput. In addition, an analysis of the position of the sternal notch towards the thyroid notch is helpful. Should the diagnosis remain unclear, a simple anterior-posterior X-ray is normally sufficient to resolve the problem.
In combinations of laterocaput and laterocollis, the angles between the thoracic spine and the cervical spine and/or between the cervical spine and the skull typically provide sufficient information in order to determine the distribution of botulinum toxin dose between the two different muscle groups.

Laterocollis

From: Reichel G, Stenner A, Jahn A. The phenomenology of cervical dystonia. Fortschr Neurol Psychiatr 2009;77(5):272–7.

From: Reichel G. Cervical dystonia: A new phenomenological classification for botulinum toxin therapy. Basal Ganglia [Internet] 2011;1(1):5–12.

From: Reichel G, Stenner A, Jahn A. The phenomenology of cervical dystonia. Fortschr Neurol Psychiatr 2009;77(5):272–7.
Scalenus posterior/medius/anterior Posterior: Max 25 u Botox; 1x40-60 - Max 100 u Dysport
Trapezius 2 x 7.5-10 u Max 50 u Botox; 2 x 30-40 max 200 u Dysport
Alternative scheme and muscles for injection shown: (After: Jost WH, Tatu L. Selection of Muscles for Botulinum Toxin Injections in Cervical Dystonia. Mov Disord Clin Pract 2015;2(3):224–6)
Ipsilateral to side of lateroflexion
Laterocaput
From: Reichel G, Stenner A, Jahn A. The phenomenology of cervical dystonia. Fortschr Neurol Psychiatr 2009; 77: 272–7.
TREATMENT (After: Jost WH, Tatu L. Selection of Muscles for Botulinum Toxin Injections in Cervical Dystonia. Mov Disord Clin Pract 2015;2(3):224–6)
Ipsilateral to side of lateroflexion
- Sternocleidomastoid
- Trapezius (Descending portion)
- Splenius capitis
- Semispinalis capitis (secondary)
- Longissimus capitis (secondary)
- Levator scapulae (secondary)
7. Additionally, obliquus capitis superior may be injected.
Lateral shift is always a result of laterocollis to one side and laterocaput to the opposite contralateral side: Thus, muscles attached to the cervical spine on the side of the shift, and the muscles attached to the skull on the opposing side, require treatment.
The neck and head (line A) are oriented in opposite directions;
 |
 |
From: Reichel G, Stenner A, Janh A. [Cervical dystonia: clinical-radiological correlations and recommendations for the correction of botulinum therapy]. Zh Nevrol Psikhiatr Im S S Korsakova. 2012;112(1):73-9. Russian. PMID: 22678680.

From: Reichel G. Cervical dystonia: A new phenomenological classification for botulinum toxin therapy. Basal Ganglia [Internet] 2011;1(1):5–12. Available from: http://dx.doi.org/10.1016/j.baga.2011.01.001